
Thursday, March 24, 2011
Thursday, March 17, 2011
CASE STUDY
A. Personal Data Summary
This are the following personal data gathered by the client child:
Name: Jesmar Abellanosa
Nick name: Botchok
Age: 7yrs. Old
Gender: Male
B-day: Nov. 27, 2004
Birth Place: Caloocan City
Sibling: None
Ordinal Position: First
Father Name: Randy Abellanosa
Occupation: Construction Worker
Mother Name: Gina Mapalad
Occupation: N/A
Temporary Guardian: Marilou Emperado
Occupation: Dress Maker
Educational Attainment of the child: Grade 1
B. Joining Process
This therapeutic approach is about to my client child, he is my neighborhood who had aggressive attitude and attention seeker it is according to the father and to their maid of my client child. His name is Jesmar abellanosa and he is 7yrs. Old. He referred to me by their maid and she is also my neighborhood. According to the father of my client child, jesmar is very aggressive child because he bullying his playmates and even his classmates without hurting him
C. Presenting Problem
Based on the Father of the client child, his son is not good in his study because he entered his son twice in Grade 1, but he think that his son doesn’t learned because every time he teach his son, the child did not listen to him and he was noticed that his son doesnt know how to count numbers and read. And sometimes the child imitate what he see or hear around him,like he imitate bad words.The problem of the child is, he have an attention seeker. He trying to get the attention of his family in the way of asking question like what is this? What are you doing? and etc.
In the school, based on his teacher of the client child always did not finished his work instead he wants to play than to do his work in school. And the other problem that I gathered to his teacher is, the child is very aggressive he often fights his classmates.
D. Psychosocial history
D.1 Timeline
When the client child was 1yr. old his parents decided to have separation because the reason of they are always fighting to each other. After the separation, the other of the client child left without any letter to his X husband. The client child stayed at his father together with his tita. They take care the child but didn’t give all the needs of the child especially the love and care that came to his mom. At the age of 5yrs. Old, the child entered in preschool with the supports of his father together with his Tita. After in preschool, he entered in Grade 1, in that level the child are not already know how to write his name. Therefore the child is not ready in formal schooling and in this time the child is more aggressive even he was at their home and in the school. He makes fun to his playmates and even with his classmates.
Now, the client child was in the grade 1 again because there are so many reason, he failed his academic subjects last year and also because of his aggressive behavior. Last, there is no guide with his parents or guardian because they are busy in their work. Therefore, they don’t have time no the child.
D.2 Genogram

Based on this genogram, there is three generation about the family of the child. We can observe that the line between the child and his mother and grandparents are broken because the client child was not closed to them. Due to the reason that when the client child was born, he doesn’t see his mom even with his grandparents too. The reason why, because his parents decided to separate to each other. His parents always fighting to each other. Therefore, the relationship between the child and his mother are not good.
In the other hand, the relationship between the child and his father are good because his father raise him up until now. But his grandparents in his father side, we can say that the client child was not also closed to them because he doesn’t see them like with his grandparents in his mother side.
D.3 Sociogram

In this diagram, there is no any arrow between the child and his mother because since the child was born, he did not see his mother until now, so that the client child was not close to his mother. When he is 1yr. old his parents decided to have separation. Therefore, we could say that the client child and his dad were closed to each other together with his Tita. Due to the reason that his Tita served as his mother and guardian. His Tita have three son but the two of them were not close of the client child because they are not always in their house. They are always busy in their work. On the other hand, the youngest son found closer to the client child for he always stayed at their home unlike the two and even the husband of his Tita is not close to the client child because he is busy in his work too.
At home(3likes and dislike)
3 likes
1) Morella
2) Nining
3) Carl
3 dislikes
1) Lyza
2) Stephane
3) Jb
In the school
3Likes
1) Jonna
2) Jm
3) Rayven
3dislikes
1) Ronnie
2) Jerome
3) christian
D.4 Personal Dynamics (self-mastery)
The relationship between my client child and with his family is not totally good because not all of them are his close. They don’t want to play with him because they are busy in their work. But sometimes if his father is not busy he spends time to his son. Therefore, the closeness between the child and his father appeared
On the other hand, the relationship between my client child and the two son of his tita is not good. The closeness between them is not appear because based on what I observed his cousins are not interested to play with him. They are focus in their work and they don’t have a time to the child.
D.5 Personal Dynamics (relationship of the child toward to his family)
The relationship between the client child and his Family are not totally good because not all of the adults around him are wants to playing with his or guide to him. The reason is, they are busy in their work but sometimes if his father is not busy he spend time to his son. Therefore, there is closeness between the child and his father. While in the relationship between the child and the two son of his Tita, I can say that the closeness are not there because based on what I observed, the two son of his Tita are not interested to play with the child or they don’t care about the child. They are focused in their work.
D.6 Personal dynamics (Particularly in Action)
Based on the information that I gathered to my client child. At their home, the child is capable in playing with his favorite toys which is the robot and cars. He also capable in watching television, watching his favorite cartoon characters which is “ben10”. He like “Ben10” because it is very unique than the other cartoon characters based on him. He also said that, “ben10” transform in different characters and every character there is a power.
In the school, the client child are capable in drawing, he always drew a house, trees and children playing “habul-habulan” in the garden
E. Theoretical framework
I think the theory that I can relate to the problem of my client child is the “ social learning theory” develop by Albert bandura it is about the imitation. Children imitate what they see around them. Like the problem of my client child he imitate what he see and heard around him. Let say for example that he did is, he heard bad word to his father and after that he imitate that.
The principles that I can also relate again to the another problem of my client child is the principles of motivation which is the learning is most effective when an individual is ready to learn. In the case of my client child, when he was entered in formal schooling the child is not ready to learn because the wants to play than to do his task.
F. Prognosis
I think why my client child became aggressive because the child did not guide by his parents/guardian because there are busy in their work. Aggressive acts become more frequent during children’s play in the preschool years. Jesmar fight his classmates or playmates without hurting him. This kind of aggression is not really directed toward the other child but maybe it is a way of expressing frustrations. Jesmar sometimes lack of attention because he trying to get the attention of his family. In this situation I think he act like that because his family are not spending time to him and sometimes the child feel isolated. The other problem of my client child is he imitate badwords,in that attitude i think he acting like that because the adults around him in not aware to the possible result to the behavior of the child.
G. Theoretical plan
1) At the end of my case study, my client child is able to build knowledge in order for him to know his self, recognize alphabet and even numbers and Recognizing colors.
2) At the end of my case study, my client child is able to build reading skill, communication skill and language skill
3)At the end of my case study, my client child is able to build the following attitudes, being friendly towards to his peers and adults around him, Recognizing good and bad things.
H. Therapeutic Intervention

I. Therapeutic Progress

J. Therapeutic result
Aggression is a one problem of my client child and it is very difficult for me to socialize with him because sometimes he did not participate to e especially when i gave an activities to him. Every time that I gave an activities he always ask "Why i need to do this ?I want to play with my friends". In this reaction, I need to do something to get the attention of my client child. I was 'uto-uto" him to participate him and later on the child was participate to me. And from the activities that I gave to him, there's an improvement to him especially his knowledge and skill. in knowledge, the child can already recognize alphabets and numbers by showing flashcards to him but sometimes he forgot what is that. In term of reading skill, the child already know how to read especially in Tagalog but in English, i can say that the child was not interested to read English word because it is hard to him to understand what the word is. And I think the other reason is the progress of his learning capability is not so fast. So that, we need more time to teach the child on how to read especially in English. And i Think encouragement is important in that problem of the child.
K. label the summary,conclusion and recommendation
Summary
My client child is come from the broken family and he is the only child. According to the father of my client child is aggressive and have a attention seeker. Aggressive because the child fight and bullying his peers without hurting him, Sometimes he also imitate what he see and hear around him like he imitate bad words or something not good. Jesmar was not good in his academic because the progress of his learning is late. He cannot recognize letters and he doesn’t know how to read even his skill are not develop and the attitude that he need to achieve are establish. And the relationship of my client child towards to his family is not good because they don’t have a time to socialize with him. All of the adults around him are almost busy.
The theory that I can relate to the problem of my client child is the theory of Albert bandura which is the ‘Social learning theory”. Where in my client child imitate bad words or anything he can see around him.
In the Intervention that I gave to him, I can say that it is help to the child to develop or enhance his knowledge, skill and even his attitude. The parents are also involved to the progress of the child to monitor and guide the child.
Recommendation
I recommend to the family of my client child is to continue the activity in order to enhance and to develop more the knowledge,kill and the attitude of the child.
To lessen the misbehavior of the child I suggest that to the family of the child they need to spend time and guide him. It is very important to the progress of the child. And I also suggest that if they are really busy to their work and they don’t have time to the child. There is another way to guide or monitor the child by getting tutor. In that way, the child help to develop his learning abilities and to improve his skills.
L. Implication
Teacher can gain an understanding of the whole child in the context of the child's total environment by involving families in the assessment process.
Teacher as problem solver use a process that includes acquiring information, considering alternatives evaluating outcomes and applying this feedback to ongoing program. And as future teacher we should guide and teach our pupils in order for them to learn and we should also aware to the possible behavior of our pupils. teacher should give the needs of our students and encourage them to do their task or responsibility in order for them to success. Teacher should prepare the environment for children to learn through active exploration and interaction with adults and other children.
This are the following personal data gathered by the client child:
Name: Jesmar Abellanosa
Nick name: Botchok
Age: 7yrs. Old
Gender: Male
B-day: Nov. 27, 2004
Birth Place: Caloocan City
Sibling: None
Ordinal Position: First
Father Name: Randy Abellanosa
Occupation: Construction Worker
Mother Name: Gina Mapalad
Occupation: N/A
Temporary Guardian: Marilou Emperado
Occupation: Dress Maker
Educational Attainment of the child: Grade 1
B. Joining Process
This therapeutic approach is about to my client child, he is my neighborhood who had aggressive attitude and attention seeker it is according to the father and to their maid of my client child. His name is Jesmar abellanosa and he is 7yrs. Old. He referred to me by their maid and she is also my neighborhood. According to the father of my client child, jesmar is very aggressive child because he bullying his playmates and even his classmates without hurting him
C. Presenting Problem
Based on the Father of the client child, his son is not good in his study because he entered his son twice in Grade 1, but he think that his son doesn’t learned because every time he teach his son, the child did not listen to him and he was noticed that his son doesnt know how to count numbers and read. And sometimes the child imitate what he see or hear around him,like he imitate bad words.The problem of the child is, he have an attention seeker. He trying to get the attention of his family in the way of asking question like what is this? What are you doing? and etc.
In the school, based on his teacher of the client child always did not finished his work instead he wants to play than to do his work in school. And the other problem that I gathered to his teacher is, the child is very aggressive he often fights his classmates.
D. Psychosocial history
D.1 Timeline

When the client child was 1yr. old his parents decided to have separation because the reason of they are always fighting to each other. After the separation, the other of the client child left without any letter to his X husband. The client child stayed at his father together with his tita. They take care the child but didn’t give all the needs of the child especially the love and care that came to his mom. At the age of 5yrs. Old, the child entered in preschool with the supports of his father together with his Tita. After in preschool, he entered in Grade 1, in that level the child are not already know how to write his name. Therefore the child is not ready in formal schooling and in this time the child is more aggressive even he was at their home and in the school. He makes fun to his playmates and even with his classmates.
Now, the client child was in the grade 1 again because there are so many reason, he failed his academic subjects last year and also because of his aggressive behavior. Last, there is no guide with his parents or guardian because they are busy in their work. Therefore, they don’t have time no the child.
D.2 Genogram

Based on this genogram, there is three generation about the family of the child. We can observe that the line between the child and his mother and grandparents are broken because the client child was not closed to them. Due to the reason that when the client child was born, he doesn’t see his mom even with his grandparents too. The reason why, because his parents decided to separate to each other. His parents always fighting to each other. Therefore, the relationship between the child and his mother are not good.
In the other hand, the relationship between the child and his father are good because his father raise him up until now. But his grandparents in his father side, we can say that the client child was not also closed to them because he doesn’t see them like with his grandparents in his mother side.
D.3 Sociogram

In this diagram, there is no any arrow between the child and his mother because since the child was born, he did not see his mother until now, so that the client child was not close to his mother. When he is 1yr. old his parents decided to have separation. Therefore, we could say that the client child and his dad were closed to each other together with his Tita. Due to the reason that his Tita served as his mother and guardian. His Tita have three son but the two of them were not close of the client child because they are not always in their house. They are always busy in their work. On the other hand, the youngest son found closer to the client child for he always stayed at their home unlike the two and even the husband of his Tita is not close to the client child because he is busy in his work too.
At home(3likes and dislike)
3 likes
1) Morella
2) Nining
3) Carl
3 dislikes
1) Lyza
2) Stephane
3) Jb
In the school
3Likes
1) Jonna
2) Jm
3) Rayven
3dislikes
1) Ronnie
2) Jerome
3) christian
D.4 Personal Dynamics (self-mastery)
The relationship between my client child and with his family is not totally good because not all of them are his close. They don’t want to play with him because they are busy in their work. But sometimes if his father is not busy he spends time to his son. Therefore, the closeness between the child and his father appeared
On the other hand, the relationship between my client child and the two son of his tita is not good. The closeness between them is not appear because based on what I observed his cousins are not interested to play with him. They are focus in their work and they don’t have a time to the child.
D.5 Personal Dynamics (relationship of the child toward to his family)
The relationship between the client child and his Family are not totally good because not all of the adults around him are wants to playing with his or guide to him. The reason is, they are busy in their work but sometimes if his father is not busy he spend time to his son. Therefore, there is closeness between the child and his father. While in the relationship between the child and the two son of his Tita, I can say that the closeness are not there because based on what I observed, the two son of his Tita are not interested to play with the child or they don’t care about the child. They are focused in their work.
D.6 Personal dynamics (Particularly in Action)
Based on the information that I gathered to my client child. At their home, the child is capable in playing with his favorite toys which is the robot and cars. He also capable in watching television, watching his favorite cartoon characters which is “ben10”. He like “Ben10” because it is very unique than the other cartoon characters based on him. He also said that, “ben10” transform in different characters and every character there is a power.
In the school, the client child are capable in drawing, he always drew a house, trees and children playing “habul-habulan” in the garden
E. Theoretical framework
I think the theory that I can relate to the problem of my client child is the “ social learning theory” develop by Albert bandura it is about the imitation. Children imitate what they see around them. Like the problem of my client child he imitate what he see and heard around him. Let say for example that he did is, he heard bad word to his father and after that he imitate that.
The principles that I can also relate again to the another problem of my client child is the principles of motivation which is the learning is most effective when an individual is ready to learn. In the case of my client child, when he was entered in formal schooling the child is not ready to learn because the wants to play than to do his task.
F. Prognosis
I think why my client child became aggressive because the child did not guide by his parents/guardian because there are busy in their work. Aggressive acts become more frequent during children’s play in the preschool years. Jesmar fight his classmates or playmates without hurting him. This kind of aggression is not really directed toward the other child but maybe it is a way of expressing frustrations. Jesmar sometimes lack of attention because he trying to get the attention of his family. In this situation I think he act like that because his family are not spending time to him and sometimes the child feel isolated. The other problem of my client child is he imitate badwords,in that attitude i think he acting like that because the adults around him in not aware to the possible result to the behavior of the child.
G. Theoretical plan
1) At the end of my case study, my client child is able to build knowledge in order for him to know his self, recognize alphabet and even numbers and Recognizing colors.
2) At the end of my case study, my client child is able to build reading skill, communication skill and language skill
3)At the end of my case study, my client child is able to build the following attitudes, being friendly towards to his peers and adults around him, Recognizing good and bad things.
H. Therapeutic Intervention

I. Therapeutic Progress

J. Therapeutic result
Aggression is a one problem of my client child and it is very difficult for me to socialize with him because sometimes he did not participate to e especially when i gave an activities to him. Every time that I gave an activities he always ask "Why i need to do this ?I want to play with my friends". In this reaction, I need to do something to get the attention of my client child. I was 'uto-uto" him to participate him and later on the child was participate to me. And from the activities that I gave to him, there's an improvement to him especially his knowledge and skill. in knowledge, the child can already recognize alphabets and numbers by showing flashcards to him but sometimes he forgot what is that. In term of reading skill, the child already know how to read especially in Tagalog but in English, i can say that the child was not interested to read English word because it is hard to him to understand what the word is. And I think the other reason is the progress of his learning capability is not so fast. So that, we need more time to teach the child on how to read especially in English. And i Think encouragement is important in that problem of the child.
K. label the summary,conclusion and recommendation
Summary
My client child is come from the broken family and he is the only child. According to the father of my client child is aggressive and have a attention seeker. Aggressive because the child fight and bullying his peers without hurting him, Sometimes he also imitate what he see and hear around him like he imitate bad words or something not good. Jesmar was not good in his academic because the progress of his learning is late. He cannot recognize letters and he doesn’t know how to read even his skill are not develop and the attitude that he need to achieve are establish. And the relationship of my client child towards to his family is not good because they don’t have a time to socialize with him. All of the adults around him are almost busy.
The theory that I can relate to the problem of my client child is the theory of Albert bandura which is the ‘Social learning theory”. Where in my client child imitate bad words or anything he can see around him.
In the Intervention that I gave to him, I can say that it is help to the child to develop or enhance his knowledge, skill and even his attitude. The parents are also involved to the progress of the child to monitor and guide the child.
Recommendation
I recommend to the family of my client child is to continue the activity in order to enhance and to develop more the knowledge,kill and the attitude of the child.
To lessen the misbehavior of the child I suggest that to the family of the child they need to spend time and guide him. It is very important to the progress of the child. And I also suggest that if they are really busy to their work and they don’t have time to the child. There is another way to guide or monitor the child by getting tutor. In that way, the child help to develop his learning abilities and to improve his skills.
L. Implication
Teacher can gain an understanding of the whole child in the context of the child's total environment by involving families in the assessment process.
Teacher as problem solver use a process that includes acquiring information, considering alternatives evaluating outcomes and applying this feedback to ongoing program. And as future teacher we should guide and teach our pupils in order for them to learn and we should also aware to the possible behavior of our pupils. teacher should give the needs of our students and encourage them to do their task or responsibility in order for them to success. Teacher should prepare the environment for children to learn through active exploration and interaction with adults and other children.
Wednesday, March 9, 2011
CASE STUDY
A. Personal Data Summary
This are the following personal data gathered by the client child:
Name: Jesmar Abellanosa
Nick name: Botchok
Age: 7yrs. Old
Gender: Male
B-day: Nov. 27, 2004
Birth Place: Caloocan City
Sibling: None
Ordinal Position: First
Father Name: Randy Abellanosa
Occupation: Construction Worker
Mother Name: Gina Mapalad
Occupation: N/A
Temporary Guardian: Marilou Emperado
Occupation: Dress Maker
Educational Attainment of the child: Grade 1
B. Joining Process
This therapeutic approach is about to my client child, he is my neighborhood who had aggressive attitude and attention seeker it is according to the father and to their maid of my client child. His name is Jesmar abellanosa and he is 7yrs. Old. He referred to me by their maid and she is also my neighborhood. According to the father of my client child, jesmar is very aggressive child because he bullying his playmates and even his classmates without hurting him
C. Presenting Problem
Based on the Father of the client child, his son is not good in his study because he entered his son twice in Grade 1, but he think that his son doesn’t learned because every time he teach his son, the child did not listen to him and he was noticed that his son did not know how to count numbers and read.
In the school, based on his teacher of the client child always did not finished his work instead he wants to play than to do his work in school. And the other problem that I gathered to his teacher is, the child is very aggressive he often fights his classmates.
D. Psychosocial history
D.1 Timeline
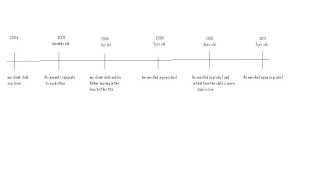
2004- Clien child was born
2005-His parents separate to each other
2009-he entered In preschool
2010-he entered in grade 1 and he became more aggressive
2011-he enrolled again in grade 1
When the client child was 1yr. old his parents decided to have separation because the reason of they are always fighting to each other. After the separation, the other of the client child left without any letter to his X husband. The client child stayed at his father together with his tita. They take care the child but didn’t give all the needs of the child especially the love and care that came to his mom. At the age of 5yrs. Old, the child entered in preschool with the supports of his father together with his Tita. After in preschool, he entered in Grade 1, in that level the child are not already know how to write his name. Therefore the child is not ready in formal schooling and in this time the child is more aggressive even he was at their home and in the school. He makes fun to his playmates and even with his classmates.
Now, the client child was in the grade 1 again because there are so many reason, he failed his academic subjects last year and also because of his aggressive behavior. Last, there is no guide with his parents or guardian because they are busy in their work. Therefore, they don’t have time no the child.
D.2 Genogram
Based on this genogram, there is three generation about the family of the child. We can observe that the line between the child and his mother and grandparents are broken because the client child was not closed to them. Due to the reason that when the client child was born, he doesn’t see his mom even with his grandparents too. The reason why, because his parents decided to separate to each other. His parents always fighting to each other. Therefore, the relationship between the child and his mother are not good.
In the other hand, the relationship between the child and his father are good because his father raise him up until now. But his grandparents in his father side, we can say that the client child was not also closed to them because he doesn’t see them like with his grandparents in his mother side.
D.3 Sociogram
In this diagram, there is no any arrow between the child and his mother because since the child was born, he did not see his mother until now, so that the client child was not close to his mother. When he is 1yr. old his parents decided to have separation. Therefore, we could say that the client child and his dad were closed to each other together with his Tita. Due to the reason that his Tita served as his mother and guardian. His Tita have three son but the two of them were not close of the client child because they are not always in their house. They are always busy in their work. On the other hand, the youngest son found closer to the client child for he always stayed at their home unlike the two and even the husband of his Tita is not close to the client child because he is busy in his work too.
At home(3likes and dislike)
3 likes
1) Morella
2) Nining
3) Carl
3 dislikes
1) Lyza
2) Stephane
3) Jb
In the school
3Likes
1) Jonna
2) Jm
3) Rayven
3dislikes
1) Ronnie
2) Jerome
3) christian
D.4 Personal Dynamics (self-mastery)
The relationship between my client child and with his family is not totally good because not all of them are his close. They don’t want to play with him because they are busy in their work. But sometimes if his father is not busy he spends time to his son. Therefore, the closeness between the child and his father appeared
On the other hand, the relationship between my client child and the two son of his tita is not good. The closeness between them is not appear because based on what I observed his cousins are not interested to play with him. They are focus in their work and they don’t have a time to the child.
D.5 Personal Dynamics (relationship of the child toward to his family)
The relationship between the client child and his Family are not totally good because not all of the adults around him are wants to playing with his or guide to him. The reason is, they are busy in their work but sometimes if his father is not busy he spend time to his son. Therefore, there is closeness between the child and his father. While in the relationship between the child and the two son of his Tita, I can say that the closeness are not there because based on what I observed, the two son of his Tita are not interested to play with the child or they don’t care about the child. They are focused in their work.
D.6 Personal dynamics (Particularly in Action)
Based on the information that I gathered to my client child. At their home, the child is capable in playing with his favorite toys which is the robot and cars. He also capable in watching television, watching his favorite cartoon characters which is “ben10”. He like “Ben10” because it is very unique than the other cartoon characters based on him. He also said that, “ben10” transform in different characters and every character there is a power.
In the school, the client child are capable in drawing, he always drew a house, trees and children playing “habul-habulan” in the garden
E. Theoretical framework
I think the theory that I can relate to the problem of my client child is the “ social learning theory” develop by Albert bandura it is about the imitation. Children imitate what they see around them. Like the problem of my client child he imitate what he see and heard around him. Let say for example that he did is, he heard bad word to his father and after that he imitate that.
The principles that I can also relate again to the another problem of my client child is the principles of motivation which is the learning is most effective when an individual is ready to learn. In the case of my client child, when he was entered in formal schooling the child is not ready to learn because the wants to play than to do his task.
F. Prognosis
I think why my client child became aggressive because the child did not guide by his parents/guardian because there are busy in their work. Aggressive acts become more frequent during children’s play in the preschool years. Jesmar fight his classmates or playmates without hurting him. This kind of aggression is not really directed toward the other child but maybe it is a way of expressing frustrations. Jesmar sometimes lack of attention because he trying to get the attention of his family. In this situation I think he act like that because his family are not spending time to him and sometimes the child feel isolated.
To lessen the misbehavior of the child I suggest that to the family of the child they need to spend time and guide him. It is very important to the progress of the child. And I also suggest that if they are really busy to their work and they don’t have time to the child. There is another way to guide or monitor the child by getting tutor. In that way, the child help to develop his learning abilities and to improve his skills.
This are the following personal data gathered by the client child:
Name: Jesmar Abellanosa
Nick name: Botchok
Age: 7yrs. Old
Gender: Male
B-day: Nov. 27, 2004
Birth Place: Caloocan City
Sibling: None
Ordinal Position: First
Father Name: Randy Abellanosa
Occupation: Construction Worker
Mother Name: Gina Mapalad
Occupation: N/A
Temporary Guardian: Marilou Emperado
Occupation: Dress Maker
Educational Attainment of the child: Grade 1
B. Joining Process
This therapeutic approach is about to my client child, he is my neighborhood who had aggressive attitude and attention seeker it is according to the father and to their maid of my client child. His name is Jesmar abellanosa and he is 7yrs. Old. He referred to me by their maid and she is also my neighborhood. According to the father of my client child, jesmar is very aggressive child because he bullying his playmates and even his classmates without hurting him
C. Presenting Problem
Based on the Father of the client child, his son is not good in his study because he entered his son twice in Grade 1, but he think that his son doesn’t learned because every time he teach his son, the child did not listen to him and he was noticed that his son did not know how to count numbers and read.
In the school, based on his teacher of the client child always did not finished his work instead he wants to play than to do his work in school. And the other problem that I gathered to his teacher is, the child is very aggressive he often fights his classmates.
D. Psychosocial history
D.1 Timeline
2004- Clien child was born
2005-His parents separate to each other
2009-he entered In preschool
2010-he entered in grade 1 and he became more aggressive
2011-he enrolled again in grade 1
When the client child was 1yr. old his parents decided to have separation because the reason of they are always fighting to each other. After the separation, the other of the client child left without any letter to his X husband. The client child stayed at his father together with his tita. They take care the child but didn’t give all the needs of the child especially the love and care that came to his mom. At the age of 5yrs. Old, the child entered in preschool with the supports of his father together with his Tita. After in preschool, he entered in Grade 1, in that level the child are not already know how to write his name. Therefore the child is not ready in formal schooling and in this time the child is more aggressive even he was at their home and in the school. He makes fun to his playmates and even with his classmates.
Now, the client child was in the grade 1 again because there are so many reason, he failed his academic subjects last year and also because of his aggressive behavior. Last, there is no guide with his parents or guardian because they are busy in their work. Therefore, they don’t have time no the child.
D.2 Genogram
Based on this genogram, there is three generation about the family of the child. We can observe that the line between the child and his mother and grandparents are broken because the client child was not closed to them. Due to the reason that when the client child was born, he doesn’t see his mom even with his grandparents too. The reason why, because his parents decided to separate to each other. His parents always fighting to each other. Therefore, the relationship between the child and his mother are not good.
In the other hand, the relationship between the child and his father are good because his father raise him up until now. But his grandparents in his father side, we can say that the client child was not also closed to them because he doesn’t see them like with his grandparents in his mother side.
D.3 Sociogram
In this diagram, there is no any arrow between the child and his mother because since the child was born, he did not see his mother until now, so that the client child was not close to his mother. When he is 1yr. old his parents decided to have separation. Therefore, we could say that the client child and his dad were closed to each other together with his Tita. Due to the reason that his Tita served as his mother and guardian. His Tita have three son but the two of them were not close of the client child because they are not always in their house. They are always busy in their work. On the other hand, the youngest son found closer to the client child for he always stayed at their home unlike the two and even the husband of his Tita is not close to the client child because he is busy in his work too.
At home(3likes and dislike)
3 likes
1) Morella
2) Nining
3) Carl
3 dislikes
1) Lyza
2) Stephane
3) Jb
In the school
3Likes
1) Jonna
2) Jm
3) Rayven
3dislikes
1) Ronnie
2) Jerome
3) christian
D.4 Personal Dynamics (self-mastery)
The relationship between my client child and with his family is not totally good because not all of them are his close. They don’t want to play with him because they are busy in their work. But sometimes if his father is not busy he spends time to his son. Therefore, the closeness between the child and his father appeared
On the other hand, the relationship between my client child and the two son of his tita is not good. The closeness between them is not appear because based on what I observed his cousins are not interested to play with him. They are focus in their work and they don’t have a time to the child.
D.5 Personal Dynamics (relationship of the child toward to his family)
The relationship between the client child and his Family are not totally good because not all of the adults around him are wants to playing with his or guide to him. The reason is, they are busy in their work but sometimes if his father is not busy he spend time to his son. Therefore, there is closeness between the child and his father. While in the relationship between the child and the two son of his Tita, I can say that the closeness are not there because based on what I observed, the two son of his Tita are not interested to play with the child or they don’t care about the child. They are focused in their work.
D.6 Personal dynamics (Particularly in Action)
Based on the information that I gathered to my client child. At their home, the child is capable in playing with his favorite toys which is the robot and cars. He also capable in watching television, watching his favorite cartoon characters which is “ben10”. He like “Ben10” because it is very unique than the other cartoon characters based on him. He also said that, “ben10” transform in different characters and every character there is a power.
In the school, the client child are capable in drawing, he always drew a house, trees and children playing “habul-habulan” in the garden
E. Theoretical framework
I think the theory that I can relate to the problem of my client child is the “ social learning theory” develop by Albert bandura it is about the imitation. Children imitate what they see around them. Like the problem of my client child he imitate what he see and heard around him. Let say for example that he did is, he heard bad word to his father and after that he imitate that.
The principles that I can also relate again to the another problem of my client child is the principles of motivation which is the learning is most effective when an individual is ready to learn. In the case of my client child, when he was entered in formal schooling the child is not ready to learn because the wants to play than to do his task.
F. Prognosis
I think why my client child became aggressive because the child did not guide by his parents/guardian because there are busy in their work. Aggressive acts become more frequent during children’s play in the preschool years. Jesmar fight his classmates or playmates without hurting him. This kind of aggression is not really directed toward the other child but maybe it is a way of expressing frustrations. Jesmar sometimes lack of attention because he trying to get the attention of his family. In this situation I think he act like that because his family are not spending time to him and sometimes the child feel isolated.
To lessen the misbehavior of the child I suggest that to the family of the child they need to spend time and guide him. It is very important to the progress of the child. And I also suggest that if they are really busy to their work and they don’t have time to the child. There is another way to guide or monitor the child by getting tutor. In that way, the child help to develop his learning abilities and to improve his skills.
Thursday, December 16, 2010
Mole
Management Of Learning Experiences
I learned that by doing that activity, in that way
we express our feelings or emotion by sharing to others
and I realized that everyone has a different problems and
happiness and I realized that I'm not alone.
And all the hindrances or problems that we encountered
in our life has a purpose " Why we need to experience all
of those things " but always remember that God is always
here for us to help and to guide us. All the things that
was happened in our life is also part of our lives because
God planned it for us to become strong.
I learned that by doing that activity, in that way
we express our feelings or emotion by sharing to others
and I realized that everyone has a different problems and
happiness and I realized that I'm not alone.
And all the hindrances or problems that we encountered
in our life has a purpose " Why we need to experience all
of those things " but always remember that God is always
here for us to help and to guide us. All the things that
was happened in our life is also part of our lives because
God planned it for us to become strong.
Sunday, December 12, 2010
Problem Checklist
PROBLEM CHECKLIST
Individual Problem Checklist
Emotional Concerns
feeling anxious or uptight
excessive worrying
not being able to relax
feeling panicky
unable to calm yourself down
dwelling on certain thoughts or images
fearing something terrible about to happen
avoiding certain thoughts or feelings
having strong fears
worrying about a nervous breakdown
feeling out of control
avoiding being with people
fears of being alone or abandoned
feeling guilty
having nightmares
flashbacks
troubling or painful memories
missing periods of time - can't remember
trouble remembering things
feeling numb instead of upset
feeling unreal, strange or foggy
feeling depressed or sad
being tired or lacking energy
feeling unmotivated
loss of interest in many things
having trouble concentrating
having trouble making decisions
feeling the future looks hopeless
feeling worthless or a failure
being unhappy all the time
dissatisfied with physical appearance
feeling self critical or blaming yourself
having negative thoughts
crying often
feeling empty
withdrawing inside yourself
thinking too much about death
thoughts of hurting yourself
thoughts of killing yourself
frequent mood swings
feeling resentful or angry
feeling irritable or frustrated
feeling rage
feeling like hurting someone
__________________________________________________
Behavioral and Physical Concerns
not having an appetite
eating in binges
self induced vomiting for weight control
using laxatives for weight control
eating too much
eating too little
losing weight
gaining weight
trouble sleeping
trouble falling asleep
early morning awakening
sleeping too much
sleeping too little
lack of exercise
not having leisure activities
smoking cigarettes
temper outbursts
aggressive toward others
impulsive reactions
trouble finishing things
working too hard
using alcohol too much
being alcoholic
using drugs
driving under the influence
blackouts - after drinking
_______________________________________________
Intimate Relationship Concerns
feeling misunderstood in relationship
not feeling close to partner
trouble communicating with partner
not trusting partner
lack of respect by partner
partner being secretive
lack of fairness in relationship
problems with dividing household tasks
disagreeing about children
lack of affection
unsatisfactory sexual relationship
lack of time together
lack of shared interests
jealousy in relationship
frequent arguments
trouble resolving conflict
partner being demanding and controlling
partner putting you down
violent arguments
emotional abuse in relationship
physical abuse in relationship
sexual abuse in relationship
partner having alcohol or drug problem
self or partner having an affair
feeling uncommitted to relationship
wanting to separate
discussing separating or divorce
problems with in-laws
problems with ex-partner
problems with step parents
children having special problems
_________________________________________________
Sexual Concerns
worrying about getting pregnant
having miscarriage(s)
choice of birth control
having an abortion
not able to become pregnant
not enjoying sexual affection
too tired to have sex
too anxious to have sex
feeling a lack of sexual desire
wanting to have sex more often
feeling neglected sexually
feeling used sexually
feeling unable to have orgasm
being unable to sustain an erection
feeling negatively about sex
When Growing Up to Present Time:
being physically abused - by whom?
being emotionally abused - by whom?
being sexually abused - by whom?
having an alcoholic parent - which?
having a drug abusing parent - which?
having a depressed parent - which?
having a parent with emotional problems
having parents separate or divorce
close family member dying - who?
felt neglected or unloved - by whom
having an unhappy childhood
having serious medical problems
having learning problems
having emotional problems
having attempted suicide - when?
Individual Problem Checklist
Emotional Concerns
feeling anxious or uptight
excessive worrying
not being able to relax
feeling panicky
unable to calm yourself down
dwelling on certain thoughts or images
fearing something terrible about to happen
avoiding certain thoughts or feelings
having strong fears
worrying about a nervous breakdown
feeling out of control
avoiding being with people
fears of being alone or abandoned
feeling guilty
having nightmares
flashbacks
troubling or painful memories
missing periods of time - can't remember
trouble remembering things
feeling numb instead of upset
feeling unreal, strange or foggy
feeling depressed or sad
being tired or lacking energy
feeling unmotivated
loss of interest in many things
having trouble concentrating
having trouble making decisions
feeling the future looks hopeless
feeling worthless or a failure
being unhappy all the time
dissatisfied with physical appearance
feeling self critical or blaming yourself
having negative thoughts
crying often
feeling empty
withdrawing inside yourself
thinking too much about death
thoughts of hurting yourself
thoughts of killing yourself
frequent mood swings
feeling resentful or angry
feeling irritable or frustrated
feeling rage
feeling like hurting someone
__________________________________________________
Behavioral and Physical Concerns
not having an appetite
eating in binges
self induced vomiting for weight control
using laxatives for weight control
eating too much
eating too little
losing weight
gaining weight
trouble sleeping
trouble falling asleep
early morning awakening
sleeping too much
sleeping too little
lack of exercise
not having leisure activities
smoking cigarettes
temper outbursts
aggressive toward others
impulsive reactions
trouble finishing things
working too hard
using alcohol too much
being alcoholic
using drugs
driving under the influence
blackouts - after drinking
_______________________________________________
Intimate Relationship Concerns
feeling misunderstood in relationship
not feeling close to partner
trouble communicating with partner
not trusting partner
lack of respect by partner
partner being secretive
lack of fairness in relationship
problems with dividing household tasks
disagreeing about children
lack of affection
unsatisfactory sexual relationship
lack of time together
lack of shared interests
jealousy in relationship
frequent arguments
trouble resolving conflict
partner being demanding and controlling
partner putting you down
violent arguments
emotional abuse in relationship
physical abuse in relationship
sexual abuse in relationship
partner having alcohol or drug problem
self or partner having an affair
feeling uncommitted to relationship
wanting to separate
discussing separating or divorce
problems with in-laws
problems with ex-partner
problems with step parents
children having special problems
_________________________________________________
Sexual Concerns
worrying about getting pregnant
having miscarriage(s)
choice of birth control
having an abortion
not able to become pregnant
not enjoying sexual affection
too tired to have sex
too anxious to have sex
feeling a lack of sexual desire
wanting to have sex more often
feeling neglected sexually
feeling used sexually
feeling unable to have orgasm
being unable to sustain an erection
feeling negatively about sex
When Growing Up to Present Time:
being physically abused - by whom?
being emotionally abused - by whom?
being sexually abused - by whom?
having an alcoholic parent - which?
having a drug abusing parent - which?
having a depressed parent - which?
having a parent with emotional problems
having parents separate or divorce
close family member dying - who?
felt neglected or unloved - by whom
having an unhappy childhood
having serious medical problems
having learning problems
having emotional problems
having attempted suicide - when?
Happy Thoughts
Happy thoughts
Family
God
Friends
My Inspiration
Hindrances
My Mom
Mistakes
Misunderstanding
Personal Problem
What can help you maintain these Happy Thoughts?
Trust and faith to God because every problem that we
encountered in our life has a purpose
Trust to each other
Have a better communication
Love and help each other
Respect their opinion and don’t be selfish
Always think positive even you have a problem
Family
God
Friends
My Inspiration
Hindrances
My Mom
Mistakes
Misunderstanding
Personal Problem
What can help you maintain these Happy Thoughts?
Trust and faith to God because every problem that we
encountered in our life has a purpose
Trust to each other
Have a better communication
Love and help each other
Respect their opinion and don’t be selfish
Always think positive even you have a problem
Tuesday, November 30, 2010
List of common problems that encountered by young children
Mental Problems
Psychological Disorders
Many psychological disorders first diagnosed in children involve physiological and/or genetic components. However, there are many other psychological disorders found in children without any physical causes. Disorders caused by physiological or biological problems are more likely to be identified early in life, but some of these problems are not identified until adulthood.
Mental retardation, learning disorders, communication skills disorders and pervasive developmental disorders (such as autistic disorder) appear to have biological components. Some psychologists specialize in the identification and treatment of these disorders, but they are not frequently encountered in a general psychological practice because of the need for specialized training and treatment. Therefore, they will not be discussed here. Elimination disorders are encountered in general psychological practice, but are typically seen as a symptomatic expression of other psychological problems. They will also not be discussed here.
Attention-deficit disorder and disruptive behavior disorders are quite common, and treatment is provided by psychologists to both children and parents to assist in managing these problems. Dr. franklin provides treatment for Attention-deficit hyperactive disorders, oppositional disorder and conduct disorders. These problems will be addressed here.
Separation anxiety is also described here. This problem is distinct from the other anxiety disorders, because it applies exclusively to children and adolescents. Separation anxiety also occurs frequently after some emotional stress or trauma, such as relocation or divorce, so the problem may also be connected to life stress issues frequently treated in private practice. It also occurs more frequently in children whose mothers have been diagnosed with panic disorder. This may suggest a biological component, or it may suggest that separation anxiety can be a psychosocial byproduct of the panic disorder in the parent. This problem is relatively common, and is usually treated by psychologists after the child has encountered adjustment problems with peers or in school.
Low attention and concentration levels
Children with ADHD have a great deal of difficulty filtering out unnecessary inputs. They are easily distracted and have a short attention span. Some children have problems with visual inputs and may be distracted by the movements of people or other forms. Some have difficulty with sound inputs such as people talking or background noise. Students with ADHD have greater difficulty listening to important messages when they are presented with unimportant detail. These students also have more difficulty thinking while in the presence of interesting conversation. Failure to selectively attend to small changes could explain some of the deficits observed with mixed-action, -operation, and -order-of-operation word problems (Zentall 1993). The Dunedin study explored behavioural distinctions in children with reading disabilities and/or ADHD (Pisecco, Baker, Silva et al 1996).
Impulsivity
Impulsivity is shown in the child's difficulty in withholding active responses (blurting out statements; grabbing materials). Impulsivity produces academic errors, primarily because an individual fails to wait long enough to consider alternative information, consequences, or responses. According to Silver (1990) some children have "short fuses"; they do not stop to think before acting.
Children with ADHD are also less likely to ask for help. That is, they do not request additional confirmatory information when it involves delaying action (Whalen, Henker, Collins et al 1979).
Low self-esteem
Academic and social difficulties make it very likely that children with ADHD experience a high rate of negative feedback on their abilities and a high rate of negative interactions with significant others in their environment. It is not surprising, then, that many children with ADHD also have a poor self-concept and low self-esteem (Weiss, Hechtman and Perlman 1978).
Difficulty with socialisation
In addition to academic problems, children with ADHD tend to have many difficulties in social relationships. Research has shown that hyperactive children tend to elicit negative, harsh, and conflicting interactions from both parents and teachers (Whalen, Henker and Dotemoto 1980). Children with ADHD seem to elicit similar negative reactions from peers, since they are often unpopular or rejected by their peers (Johnston, Pelham and Murphy 1985) even as young as preschool-age (Milich, Landau, Kilbey et al 1982).
Improving socialisation is appropriate for children who are deficient in social behaviour skills and experience peer relational difficulties. Training is undertaken which is designed to increase knowledge of appropriate and inappropriate social behaviours and to help children to put into practice behaviours that are appropriate. The various target skills taught may include maintaining eye contact, initiating and maintaining conversation, and sharing/cooperating. Role-play exercises with group feedback are typically used. Due to the frequency of behavioural disruptions that occur, some form of group contingency management system is usual.
Social Emotional Disorders
Early recognition of social and emotional problems in infants and preschool children is necessary for best developmental
outcomes. Social and emotional difficulties continue over time and are highly resistant to change. It is not surprising
that a strong relationship exists between childhood behavior problems, delinquency, and later criminality. If left
untreated, “early-onset” conduct problems (high rates of aggression, disobedience, oppositional behaviors and emotional
impairment) place children at high risk for persistent social and emotional problems, underachievement, school drop out
and ultimately delinquency. Research has demonstrated that a young child’s ability to learn is assured by a sense of
security and stability, and continuous relationships with adults, including their families and communities.
Early identification and intervention with social and emotional problems can have a significant impact on the developing
child in three major areas. First, brain development, important early relationships and experiences can positively affect
gene role, neural connections, and the organization of the mind, having a life-long positive effect. Positive early
experiences lay the necessary foundation for the healthy growth of future behaviors and thought development. The
development of emotional self being and social ability in the early years plays a critical part in shaping the way children
think, learn, react to challenges, and develop relationships throughout their lives.
Social and Emotional Facts
• Kindergarten teachers say that about 20 percent of children entering kindergarten do not yet have the necessary social
and emotional skills to be “ready” for school.
• Social and emotional development is important because it contributes to cognitive development.
• When children are young, the adults around them (parents, other adult caregivers, preschool teachers) are the most
important influences on their social and emotional development.
• Preschool education can support early development with long term social and emotional benefits.
Understanding Social and Emotional Behaviors
Evaluating social and emotional capability in very young children can be difficult. Accuracy of the child’s behavior
often depends upon certain variables including the age of the child, when the behavior occurs, the setting where it
occurs, and which adults are present at the time. Developmental and cultural variability, differences in adult and child
temperament, and changing behavioral expectations are some factors that make social and emotional assessment
particularly challenging. For example, one family may tolerate loud talking and throwing of play toys while another
family may tolerate only quiet voices and no throwing of objects indoors. A two-year-old who throws herself on the
floor at the supermarket and screams because she can’t have a chocolate donut will not be labeled “unusual” while an
eight-year old who does the same would be.
Very young children, for example, have to learn to understand and recognize their own feelings, but then they
increasingly learn to associate verbal labels to those feelings, to learn that others have feelings too, and to begin to
sympathize with others. As children grow older, they learn to manage their emotions to block feelings of anxiety,
sadness, or frustration, and to delay gratification in order to achieve a goal.
Children need a combination of intellectual skills, motivational qualities, and social emotional skills to succeed in school.
They must be able to understand the feelings of others, control their own feelings and behaviors, and get along with
their peers and teachers. Children need to be able to cooperate, follow directions, demonstrate self-control, and “pay
attention.” One of the most important skills that children develop is self-control - the ability to manage one’s behavior
so as to resist impulses, maintain focus, and undertake tasks even if there are other more tempting options available.
Self-control motivates the ability to take on every task, so that the outcomes are not just how children get along with
one another but also how they can focus and learn in the classroom.
Social-emotional skills include the following:
• The child is able to understand and talk about his/her own feelings.
• The child understands the perspective of others and realizes that their feelings may be different from his/her own
feelings.
• The child is able to establish relationships with adults and maintains an ongoing friendship with at least one other
child.
• The child is able to enter a group successfully.
• The child is able to engage in and stay with an activity for a reasonable amount of time with minimal adult
support.
Social and emotional development involves the achievement of a set of skills. Among them is the ability to:
• Identify and understand one’s own feelings.
• Accurately read and comprehend emotional reactions from others.
• Manage strong emotions and their expression in a constructive manner.
• Control one’s own behavior.
• Develop compassion for others.
• Establish and maintain relationships.
Social and Emotional Behaviors in Preschool
Children with social and emotional problems enter kindergarten unable to learn because they cannot pay attention,
remember information on purpose, or act socially in a school environment. The result is growing numbers of children
who are hard to manage in the classroom. These children cannot get along with each other, follow directions, and are
impulsive. They show hostility and aggression in the classroom and on the playground. The problems begin before
kindergarten. In some studies as many as 32 percent of preschoolers in Head Start programs have behavioral problems.
Children lacking social and emotional skills suggest that teachers spend too much time trying to restrain unmanageable
children and less time teaching. Early childhood teachers report that they are extremely concerned about growing
classroom management problems, and that they are unprepared to handle them. Kindergarten teachers report that more
than half of their students come to school unprepared for learning academic subjects. If these problems are not dealt
with, the result can be growing aggression, behavioral problems and, for some, delinquency and crime through the
school years and into adolescence and adulthood.
Social and Emotional Aggression
Continual physical aggression, high-school dropout rates, adolescent delinquency, and antisocial behavior have all been
associated with early childhood conduct problems. The preschool years are a vulnerable period for learning to control
development of aggression. Children who display high levels of physical aggression in elementary school are at the
highest risk for taking part in violent behaviors as adolescents.
Researchers believe that children with difficult, disruptive behavior (poor social and emotional skills) are at risk for
these later problems for at least three reasons: (1) teachers find it harder to teach them, seeing them as less socially and
academically capable, and therefore provide them with less positive feedback; (2) peers reject them, which obstructs an
important opportunity for learning and emotional support; and (3) children faced with this rejection from peers and
teachers are likely to dislike school and learning, which leads to lower school attendance and poorer outcomes.
Difficult behavior exhibits itself early, even before children begin kindergarten; the pattern of rejection and negative
experiences begins early, too. The early experience of rejection can have lasting emotional and behavioral impacts
beyond elementary school, creating the problem even more difficult to reverse.
Developing Social and Emotional Skills
Promoting social and emotional development and preventing problems caused by inadequate development is clearly
important to individuals and to society. They begin with the relationships children form with the people around them,
including parents, caregivers, and peers. One characteristic of a successful person is his or her ability to live and work
peacefully and productively with others. Social capacity is the ability to interact positively within personal and family
relationships, as well as the ability to demonstrate positive concern and consideration. Emotionally healthy children
engage in positive behaviors, develop mutual friendships, and are more likely to find acceptance from their peers.
Through play, children learn how to work in teams and cooperate with others. Their behavior and interactions influence
the way in which teachers perceive them and the way they are treated by their peers. As early as preschool, the
relationships children develop with one another can have a lasting impact on academic achievement, because they can
contribute to more positive feelings about school and eagerness to engage in classroom activities, which can, in turn,
lead to higher levels of achievement.
Social Emotional Problems and Peer Relationships
Social interaction with peers builds upon and improves the rules and customs of social interaction that children first
encounter in their families. Although many adults assume that the influence of peers on adolescents is negative, the
repercussions of peer relationships are often more positive than negative. Peer relationships can provide cognitive,
social, and physical stimulation through mutual activities and conversations. Friendships in particular can provide
emotional security and compassion and can often serve as an additional source of support outside of the family,
especially in times of crisis.
Children must be provided an emotionally secure and safe environment that prevents any form of bullying or violence,
where they can be effective learners and integrate the development of social and emotional skills within all aspects of
school life. These skills include problem-solving, coping, conflict management/resolution and understanding and
managing feelings. Gaining social and emotional skills enables children to learn from teachers, make friends, express
thoughts and feelings, and cope with frustration. These kinds of skills, in turn, directly influence cognitive learning such
as early literacy, numeracy and language skills.
Early rejection by peers has been associated with persistent academic and social difficulties in elementary school. That
is why it is important to have skilled preschool teachers who can intervene when they see children having difficulties
with peers and help the children learn how to resolve conflicts, control emotions, and respond to the feelings of others.
Social Emotional Problems in the Family
Parents and families play a huge part in determining a child’s social and emotional development. Early relationships with
parents lay the foundation on which social ability and peer relationships are built. Parents who support positive
emotional development interact with their children affectionately; show consideration for their feelings, desires and
needs; express interest in their daily activities; respect their opinions; express pride in their achievements; and provide
support during times of anxiety. This encouragement significantly raises the probability that children will develop early
emotional capability, will be better prepared to enter school, and less likely to display behavior problems at home and at
school. This is why many preschool programs include a focus on parent involvement and parenting education.
Interactions with siblings are an important part of child development. These interactions influence the course of a child’
s social and moral development, including the development of good citizenship and good character. In general, having
an encouraging relationship with parents and siblings is important to positive adolescent development. Children who
disconnect from parental influence are at particular risk for delinquent activities and psychological problems.
Social and Emotional Support
The results of early childhood social-emotional problems may be a response from child distress and suffering, difficulty
with learning, trouble with play, poor peer interactions and sibling relationships, are all warnings of future mental health
problems. Nationally, fewer than 25% of children with clinical mental health problems receive treatment. Promoting
children’s social and emotional wellbeing can help improve their physical and mental health, performance at school and
assist with behavioral problems. A range of factors impact on how children feel, including their individual family
background and the community they live in, everyone needs to work together to agree effective strategies as part of a
team.
Children might need more focused instruction on skills such as: identifying and expressing emotions; self-control; social
problem solving; initiating and maintaining interactions; cooperative responding; strategies for handling disappointment
and anger; and friendship skills. Families of infants and young toddlers might need guidance and support for helping the
very young child regulate emotions or stress and understand the emotions of others.
Parents should consult with school staff regarding the social and emotional behavioral needs of their children. Once you
have contacted the school about concerns the following steps should be taken.
• A consultation with school staff regarding classroom and/or school approaches to behavior and to develop
positive behavior supports and interventions.
• Screening, evaluation, identification and referral for children displaying emotional disturbances.
• Planning and implementing appropriate academic and other educational supports.
• Measuring progress and improvement both for individuals and also for programs.
• Interventions for students with chronic behavior and emotional needs.
• Small group and/or individual counseling for such issues as social skills, anger control, etc.
• Development of expectations such as positive behavior and intervention, prevention of violence, crisis
planning and intervention, etc.
• Coordination and referral of children and families to community service agencies, related to mental health
needs.
When children have persistent challenging behavior that is not responsive to interventions, comprehensive interventions
are developed to resolve problem behavior and support the development of new skills. The process begins with
arranging the school staff that will develop and implement the child’s individualized education plan. At the center of the
team is the family and child’s teacher or other primary caregivers. The next step is to conduct a functional assessment
to gain a better understanding of the factors that are related to the child’s engagement in challenging behavior. The
individualized educational plan includes prevention strategies to address the triggers of challenging behavior;
replacement skills that alternatives to the challenging behavior; and strategies that ensure challenging behavior is not
reinforced or maintained. The individualized education plan is designed to address home, community, and classroom
routines where challenging behavior is occurring.
Social Convention
One of the really big problems that children encounter, that
everyone encounters in the process of growing up, is that
natural phenomenon involving a new force that presents itself
within a person at the onset of puberty. We are talking about
the powerful sexual force that manifests itself at the onset of
puberty around the age of 11 or 12 in the form of sexual
desire. Associated with this force, all mixed up with it, is
the phenomenon of "finding someone physically attractive" and
"falling in love", "being in love", etc. It is all part of the
same phenomenon. In fact, people fall into love and out of
love quite easily. "Falling in love" is really a kind of
temporary bewitchment, temporary enchantment, a temporary loss
of good sense. And involved also in this same phenomenon is
everyone's need for a companion of the opposite sex. A deep-
seated need. This whole phenomenon is nature's way of
perpetuating the species. It is a phenomenon that occurs in
all species. Behind it is the possibly partially obscured or
submerged wish to couple, procreate. Sexual desire can be like
an itch that torments. It is a new force within that dogs and
afflicts one, provoked and stimulated by imagination and
fantasy. It can be a desire that cries out for satisfaction,
an itch that demands appeasement. This entire phenomenon we
are talking about presents a lot of problems and difficulties
for a person. It is a brand new experience for a child and he
may not know quite how to handle it. Parents often don't want
to talk about it, don't quite know how to talk about it, and
the child learns about it from the effects it produces on
himself. The beginning of puberty is the end of innocence.
For along with this new force comes a realization that this
force within must be managed and controlled, since if is not
controlled, one would have a society of rampant promiscuity,
fornication and adultery; indeed a society of rampant rape,
child molestation and all kinds of ugly things. A usual way of
dealing with it is the appeasement of its incessant demands
through masturbation. The force brings frustration. For
thwarted desire produces frustration. And one knows the force
must be managed. The constantly recurring desire for sexual
intercourse coupled with the knowledge that sexual intercourse
produces babies and that you are not in any way ready in life
to have the responsibility of a baby produces inner conflict.
You are faced with the desire for something you want badly but
something that you know you must not allow, something your mind
tells you would be very bad for you, that would ruin your
future, your life. You are faced with a temptation to do
something that could be like a poison pill that could destroy
you. What a dilemma! That is life. An introduction to the
real world. In addition, you know God has stated that
fornication and adultery are sins, that fornicators and
adulterers will be punished by eternal hell. Thus this new
force brings a need for self-discipline. It creates a need for
restraint where restraint is difficult. Since it will be a
number of years yet before you will be in a position to marry
and have children you are faced with the problem of dealing
with this force by denying, thwarting and managing it for a
number of years. Thus much perseverance and patience is
required. It is a difficult task. All of this represents a
continuing, day to day problem of adolescent youth. It is
youth's first real encounter with temptation and the real need
to resist it. Many in our age do not resist it. They
foolishly follow their sexual inclinations, and end up having
babies or getting abortions. Or they take birth control pills.
They become promiscuous, having sex with multiple partners.
They follow the happy, easy way and others such as parents or
government take on the responsibilities that ought to be
theirs, the responsibilities of rearing and supporting the
illegitimate children that they beget and are not in a position
to rear. By taking the easy road, indulging their base
appetites and desires at a young age, they mess up their own
lives and place an unfair burden on others. They wrong others,
including their illegitimate children who are deserving of a
legitimate mother and father and a proper upbringing. And in
following the easy road of self-indulgence they build up habits
of sexual promiscuity that they will probably carry with them
the rest of their lives, even if they should eventually get
married.
Considering the problem that adolescent youth faces in dealing
with this problem reason and sense would call for societal
customs and practices that would assist teenagers in dealing
with the problem. If a person is overweight and is trying to
lose weight one does not place a chocolate cake under his nose.
If one is seriously attempting to avoid temptation one does not
put himself into situations producing temptation. A sensible
society could help a teenager in dealing with this problem.
Common sense would require social conventions and practices
that do not allow teenage youth of opposing sex to be alone
together. Common sense would require strict chaperoning of
youth. In a moral society parents and the adult world would
insist on chaperoning of youth. A moral society would not give
youth automobiles and the freedom that our society gives them.
Our laxness in dealing with our youth reveals our lack of
morals and unconcern about our youth. A sensible and moral
society would not allow on public mass media programs that
glamorize illegitimate sex. Teenagers do what they think
everyone else is doing. If everyone else is taking the easy,
fun, self-indulgent road they will take it too. If it is
glamorized on TV and in the movies and everyone appears to be
doing it they will do it too. It may be the foolish road but
fools follow fools. They live by the "feeling" philosophy.
Let your feelings be your guide (as opposed to your mind). Do
what you want to do, what you feel like doing. Live life.
Enjoy it. Don't let sense, reason or concern for others get in
your way.
There are many who condone illicit sex. They contend that
asking people to restrain and abstain is simply asking too much
of a person. The incidence of illicit sex and illegitimate
births among teenagers in this country is very high (over 50%
for illicit sex). However, I observe that the incidence of
illicit sex among teenagers in some cultures is extremely low
(perhaps 1 or 2 percent). I am thinking of the Japanese. I
think this fact is very interesting. It suggests that it is
all in the social attitudes and values of a particular society,
all in the "want to". People can do what they want to do. It
is all about morality or lack of it. It is true that the
Christian cultures seem just unable to restrain themselves in
regard to illicit sex. I don't fault the Christian religion
itself. The Bible is very clear on the topic, the New
Testament is very clear. The problem lies in the pervasive
perversion and corruption of Christianity. Man never seems
able to stay on a straight line. He always deviates off.
Intellectual
Adaptive behavior can also be defined as the effectiveness or degree with which the individual meets the standards of personal independence and social responsibility expected of his age and social group.[1] Adaptive behavior also refers to the typical performance of individuals without disabilities in meeting environmental expectations. Adaptive behavior changes according to a person’s age, cultural expectations, and environmental demands.
Behavior scales
To determine a student’s adaptive behavior capacities, professionals focus on the student’s conceptual skills, social skills, and practical skills. To measure adaptive skills, professionals use adaptive behavior scales that have been normed on individuals with and without disabilities. Most adaptive behavior scales are completed by interviewing a parent, a teacher, or another individual who is familiar with the student’s daily activities. Students may have a combination of strengths and needs in any or all of the areas regarding conceptual, social and practical skills.
Mental retardation/intellectual disability is significantly subaverage intellectual functioning present from birth or early infancy, causing limitations in the ability to conduct normal activities of daily living.
• Mental retardation/intellectual disability (MR/ID) can be genetic or the result of a disorder that interferes with brain development.
• Most children with MR/ID do not develop noticeable symptoms until they are in preschool.
• The diagnosis is based on the results of formal testing.
• A child's life expectancy is based on the extent of mental and physical problems.
• Proper prenatal care lowers the risk of having a child with MR/ID.
• Support from many specialists, therapy, and special education help children achieve the highest level of functioning possible.
The long-used term “mental retardation” has acquired an undesirable social stigma. Because of this stigma, doctors and health care practitioners have begun replacing it with the term "intellectual disability." Because this change is recent, the term "mental retardation/intellectual disability" (MR/ID) is used to mark the transition in terminology.
MR/ID is not a specific medical disorder like pneumonia or strep throat, and it is not a mental health disorder. People with MR/ID have significantly below average intellectual functioning that limits their ability to cope with two or more activities of normal daily living (adaptive skills). These activities include the ability to communicate; live at home; take care of oneself, including making decisions; participate in leisure, social, school, and work activities; and be aware of personal health and safety.
People with MR/ID have varying degrees of impairment. While recognizing each person's individuality, doctors find it helpful to classify a person's level of functioning. Intellectual functioning levels can be based on the results of developmental quotient (DQ) tests and intelligence quotient (IQ) tests or on the level of support needed. Support is categorized as intermittent, limited, extensive, or pervasive. Intermittent means occasional support; limited means support such as a day program in a sheltered workshop; extensive means daily, ongoing support; and pervasive means a high level of support for all activities of daily living, possibly including full-time nursing care.
Based only on IQ test scores, about 3% of the total population are considered to have MR/ID. However, if classification is based on the need for support, only about 1% of people are classified as having significant mental (cognitive) limitation.
Emotional problems in children
Emotional problems in children have become more widely recognized. A child's emotional problem can become a chronic problem if it's not attended to properly and in a timely manner. Many adult emotional problems can also affect children, but these problems may not be as easily recognized in children. Some emotional problems in children can be treated quite easily, but some require long-term care that can be complicated.
Childhood Bipolar Disorder
1. Childhood bipolar disorder is an emotional problem that can affect children. This childhood emotional problem can be hard to diagnose, because its symptoms are also symptoms of many other childhood emotional problems. Common symptoms include mood swings, irritability, episodes of extreme happiness and episodes of severe depression. Childhood bipolar disorder is a serious condition and should be treated as such. Treatment most often includes a combination of medication (sometimes more than one) and behavior therapy (teaching the child how to handle certain situations better).
Childhood Depression
2. Childhood depression is an emotional problem that can affect children. This childhood emotional problem is considered serious, but it can be difficult to diagnose because its symptoms are not unique. Common symptoms include irritability, fatigue, hopelessness, social withdrawal and poor performance in school. Childhood depression is most often treated with medication and behavior therapy.
Autism
3. Autism is an emotional problem that can affect children. This childhood emotional problem is often serious and consists of three distinctive behaviors. These autism behaviors include trouble interacting socially, obsessive and competitive behavior and difficulty with nonverbal and verbal communication. Medications (often more than one) and behavioral and educational therapies and interventions are used to treat autism. Family counseling is also used to help families learn about autistic children and to help them cope.
Childhood Schizophrenia
4. Childhood schizophrenia is an emotional problem that can affect children. This emotional disorder often affects a child's ability to develop normal social, educational and emotional skills and habits. Children with emotional disorder often have difficulty performing daily tasks, think and act irrationally and have delusions and hallucinations. Childhood schizophrenia is most often treated with a variety of treatments including medications (most often antipsychotics) and psychotherapy (teaches the child to cope with the illness and its challenges).
Tourette Syndrome
5. Tourette syndrome is an emotional problem that can affect children. This emotional problem is also considered a neurological disorder. Tourette syndrome is characterized by stereotyped and repetitive vocalizations and involuntary movements referred to as tics. Tourette syndrome is most often treated with a combination of medication and psychotherapy.
Physical
A recurrent theme of this year's AAFP Scientific Assembly was the evaluation and management of behavior problems in childhood. A series of talks focused on this issue and was led off by Dr. Barbara Howard's entertaining review of common behavioral problems encountered among children between ages 0 and 5 years.[1] Dr. Howard is Assistant Professor in Pediatrics at Johns Hopkins Medical Center and Co-Director of The Center for Promotion of Child Development through Primary Care. She noted that between 25% and 50% of physician visits for pediatric problems are behavioral, and 90% of parents with a child between the ages of 2 and 4 have some concern regarding their child's behavior.
Overall, Dr. Howard stressed the importance of "state regulation" for children, and the principal elements of this regulation are a standard routine of activities during the day and night as well as a consistent parental response to children's behaviors. Children with a history of insult to the central nervous system, lead poisoning, or exposure to substances in utero are particularly prone to behavioral problems without daily routines and consistent parental feedback.
Night awakening occurs in over 80% of children between the ages of 4 and 8 months, and 23.5% of children are not able to sleep for 6 consecutive hours at age 5 months.[2] New or problem night awakening frequently occurs after a change in the day's routine or some other stress. Dr. Howard recommends limiting naps to 2 hours per day and setting up bedtime routines. She then said, "Here comes the hard part: You have to let your baby cry a little bit." Dr. Howard recommends allowing the baby to cry for 5-10 minutes to help establish more mature sleep patterns.
Thumbsucking is a common practice among children and "may be a means of consoling themselves and also may improve gut motility and constipation," according to Dr. Howard. Nonetheless, thumbsucking may be less socially acceptable to some. "Who complains about thumbsucking?" asked Dr. Howard, "Grandma!"
Thumbsucking affects up to 31% of children and usually peaks between 1 and 2 years of age.[3] Parents should be relieved to learn that it generally does not affect dentition among children under the age of 6. For older children who continue to suck their thumbs, Dr. Howard recommends bribery or the use of thumb paint in a motivated child to dissuade thumbsucking.
Many toddlers may exhibit behavioral problems around mealtime, and Dr. Howard noted that this is probably "because autonomy is more important than hunger" during this stage of development. She discourages parents from chasing the toddler with food or bribing the child to encourage better eating habits. Instead, she recommends placement of nutritious finger foods on a low-lying table for the child to consume as desired. The child may be excused from the table at mealtime if he or she asks. Dr. Howard says that children will usually be drawn to the social experience of the mealtime table with the family after approximately 1 week of this therapy.
Dr. Howard closed with a discussion of toilet training, noting that "many children in other parts of the world begin toilet training by 1 year of age." However, children in the United States are generally encouraged to use the toilet only after they are able to control micturition and bowel movements to some extent and have full mobility. Dr. Howard stated that "there is no reason to start toilet training in a constipated kid" and recommends dietary fiber as a first-line agent to assure regularity. She also uses polyethylene glycol for children who refuse to eat fiber. She has had success using a strategy of room restriction for children having difficulty with toilet training. This strategy involves limitation of the child's movement to one room in the house (the room with the potty) until the child has a bowel movement. She noted that this strategy usually provides positive results within 2 days.
Colic is one of the most difficult behavioral problems to manage as a parent, and it warranted a separate lecture by Dr. Thomas Irons, Professor of Pediatrics at East Carolina University.[4] "I became interested in colic when I didn't know what to do about it with my own son," confessed Dr. Irons. He used the classic "rule of 3's" in defining colic as periods of intense crying for more than 3 hours per day on at least 3 days per week. He compared these statistics with an estimate that "the average baby cries an hour and three quarters per day." Colic generally resolves by 3 months of age. Dr. Irons noted that while no one treatment is effective for colic, research on therapy has demonstrated a placebo response rate of approximately 60%.[5] He encouraged parents to "take heart in the placebo effect" through treatments lacking a significant harmful potential for the baby, such as simethicone drops. Besides education and support from their family doctor, both Dr. Irons and Dr. Howard recommended "the 5 S's" as techniques which may help parents with crying infants:
• Swaddling, especially in combination with carrying the baby for a minimum of 3 hours per day;
• Side or prone positioning while the baby is being held;
• Shush -- use white noise to calm the baby;
• Sucking a pacifier; and
• Swing -- activating the vestibular system through a swing may reduce crying. Per Dr. Irons, "Run [the swing] as fast as it'll operate. Wind it up and let 'em go!"
Dr. Irons also noted some success associated with whey hydrosylate formula among children with colic who had received cow milk-based formula.[6] Parents may consider changing to this formula if their colicky infant is being bottle-fed. Dr. Howard suggested eliminating milk and cruciform vegetables from the mother's diet in colicky breastfed babies, as food allergy may play some role in colic.
Dr. Michelle May delivered an inspiring seminar regarding another problem behavior among children with which family physicians are all too familiar: overeating, lack of exercise, and obesity.[7] Dr. May is a family physician and the founder and medical director of Am I Hungry?, an adult weight-management program. She noted that 9 million children in the United States are overweight, and the prevalence has doubled in the last 2 decades.[8] She feels that identifying and treating pediatric obesity "is the hard stuff, and this is what we do as family physicians." Physicians should screen all children for overweight, using appropriate body mass index charts available at www.cdc.gov/growthcharts. Children above the 95th percentile for age-adjusted body mass index are considered overweight, although this should be interpreted with caution in adolescents because of varying rates of physical maturation.
"In this society, food is readily available, and there are many people with a financial interest in convincing us that we need to eat more than we do," stated Dr. May. She noted that portion sizes have increased by 25% to 50% over the last 2 decades. She also stated that "up to one third of food advertising contains misleading nutrition information," leading to a false sense of security for parents and children choosing foods poor in nutritional value. At the same time, less than half of schools offer physical education classes, and approximately 25% of children do not perform any physical activity outside of school.
While the negative societal influence on overweight in children runs deep, Dr. May relies on the fact that "children are born with the ability to regulate their own weight effortlessly." She offered the following advice for physicians counseling parents and children regarding diet:
• Don't reward eating. Do not praise or bribe toddlers for eating extra food, as this can establish a negative habit. Similarly, do not offer rewards for a clean plate at the end of the meal.
• Don't focus on ideal weight. Instead, set modest, achievable goals for overweight children.
• Monitor, but don't control. Dr. May finds that limiting dietary choices can be counterproductive, but focusing positively as a family on healthy foods produces healthier eating habits over the long term.[9]
• Don't give up on healthy foods. Dr. May has found that children may need to try a new food up to 10 times before accepting and enjoying it.
Regarding increasing activity, Dr. May suggested the following principles:
• Limit "screen time" (eg, television, computers, video games) to 2 hours per day.
• Address limitations in performing regular physical activity as a family, and strategize together how to overcome these barriers. The type of activity will vary from family to family but may be as simple as playing catch or taking a walk. Ideally, family physicians should be aware of community resources to help stimulate families to get active.
Overall, the series of lectures on children's behavior asserted the central role of family physicians in these health issues. Family doctors have the unique perspective of being able to assess the impact of family dynamics on children and counsel the family unit as a whole. These skills are highly valuable and will continue to be one of the strengths of the specialty.
Psychological Disorders
Many psychological disorders first diagnosed in children involve physiological and/or genetic components. However, there are many other psychological disorders found in children without any physical causes. Disorders caused by physiological or biological problems are more likely to be identified early in life, but some of these problems are not identified until adulthood.
Mental retardation, learning disorders, communication skills disorders and pervasive developmental disorders (such as autistic disorder) appear to have biological components. Some psychologists specialize in the identification and treatment of these disorders, but they are not frequently encountered in a general psychological practice because of the need for specialized training and treatment. Therefore, they will not be discussed here. Elimination disorders are encountered in general psychological practice, but are typically seen as a symptomatic expression of other psychological problems. They will also not be discussed here.
Attention-deficit disorder and disruptive behavior disorders are quite common, and treatment is provided by psychologists to both children and parents to assist in managing these problems. Dr. franklin provides treatment for Attention-deficit hyperactive disorders, oppositional disorder and conduct disorders. These problems will be addressed here.
Separation anxiety is also described here. This problem is distinct from the other anxiety disorders, because it applies exclusively to children and adolescents. Separation anxiety also occurs frequently after some emotional stress or trauma, such as relocation or divorce, so the problem may also be connected to life stress issues frequently treated in private practice. It also occurs more frequently in children whose mothers have been diagnosed with panic disorder. This may suggest a biological component, or it may suggest that separation anxiety can be a psychosocial byproduct of the panic disorder in the parent. This problem is relatively common, and is usually treated by psychologists after the child has encountered adjustment problems with peers or in school.
Low attention and concentration levels
Children with ADHD have a great deal of difficulty filtering out unnecessary inputs. They are easily distracted and have a short attention span. Some children have problems with visual inputs and may be distracted by the movements of people or other forms. Some have difficulty with sound inputs such as people talking or background noise. Students with ADHD have greater difficulty listening to important messages when they are presented with unimportant detail. These students also have more difficulty thinking while in the presence of interesting conversation. Failure to selectively attend to small changes could explain some of the deficits observed with mixed-action, -operation, and -order-of-operation word problems (Zentall 1993). The Dunedin study explored behavioural distinctions in children with reading disabilities and/or ADHD (Pisecco, Baker, Silva et al 1996).
Impulsivity
Impulsivity is shown in the child's difficulty in withholding active responses (blurting out statements; grabbing materials). Impulsivity produces academic errors, primarily because an individual fails to wait long enough to consider alternative information, consequences, or responses. According to Silver (1990) some children have "short fuses"; they do not stop to think before acting.
Children with ADHD are also less likely to ask for help. That is, they do not request additional confirmatory information when it involves delaying action (Whalen, Henker, Collins et al 1979).
Low self-esteem
Academic and social difficulties make it very likely that children with ADHD experience a high rate of negative feedback on their abilities and a high rate of negative interactions with significant others in their environment. It is not surprising, then, that many children with ADHD also have a poor self-concept and low self-esteem (Weiss, Hechtman and Perlman 1978).
Difficulty with socialisation
In addition to academic problems, children with ADHD tend to have many difficulties in social relationships. Research has shown that hyperactive children tend to elicit negative, harsh, and conflicting interactions from both parents and teachers (Whalen, Henker and Dotemoto 1980). Children with ADHD seem to elicit similar negative reactions from peers, since they are often unpopular or rejected by their peers (Johnston, Pelham and Murphy 1985) even as young as preschool-age (Milich, Landau, Kilbey et al 1982).
Improving socialisation is appropriate for children who are deficient in social behaviour skills and experience peer relational difficulties. Training is undertaken which is designed to increase knowledge of appropriate and inappropriate social behaviours and to help children to put into practice behaviours that are appropriate. The various target skills taught may include maintaining eye contact, initiating and maintaining conversation, and sharing/cooperating. Role-play exercises with group feedback are typically used. Due to the frequency of behavioural disruptions that occur, some form of group contingency management system is usual.
Social Emotional Disorders
Early recognition of social and emotional problems in infants and preschool children is necessary for best developmental
outcomes. Social and emotional difficulties continue over time and are highly resistant to change. It is not surprising
that a strong relationship exists between childhood behavior problems, delinquency, and later criminality. If left
untreated, “early-onset” conduct problems (high rates of aggression, disobedience, oppositional behaviors and emotional
impairment) place children at high risk for persistent social and emotional problems, underachievement, school drop out
and ultimately delinquency. Research has demonstrated that a young child’s ability to learn is assured by a sense of
security and stability, and continuous relationships with adults, including their families and communities.
Early identification and intervention with social and emotional problems can have a significant impact on the developing
child in three major areas. First, brain development, important early relationships and experiences can positively affect
gene role, neural connections, and the organization of the mind, having a life-long positive effect. Positive early
experiences lay the necessary foundation for the healthy growth of future behaviors and thought development. The
development of emotional self being and social ability in the early years plays a critical part in shaping the way children
think, learn, react to challenges, and develop relationships throughout their lives.
Social and Emotional Facts
• Kindergarten teachers say that about 20 percent of children entering kindergarten do not yet have the necessary social
and emotional skills to be “ready” for school.
• Social and emotional development is important because it contributes to cognitive development.
• When children are young, the adults around them (parents, other adult caregivers, preschool teachers) are the most
important influences on their social and emotional development.
• Preschool education can support early development with long term social and emotional benefits.
Understanding Social and Emotional Behaviors
Evaluating social and emotional capability in very young children can be difficult. Accuracy of the child’s behavior
often depends upon certain variables including the age of the child, when the behavior occurs, the setting where it
occurs, and which adults are present at the time. Developmental and cultural variability, differences in adult and child
temperament, and changing behavioral expectations are some factors that make social and emotional assessment
particularly challenging. For example, one family may tolerate loud talking and throwing of play toys while another
family may tolerate only quiet voices and no throwing of objects indoors. A two-year-old who throws herself on the
floor at the supermarket and screams because she can’t have a chocolate donut will not be labeled “unusual” while an
eight-year old who does the same would be.
Very young children, for example, have to learn to understand and recognize their own feelings, but then they
increasingly learn to associate verbal labels to those feelings, to learn that others have feelings too, and to begin to
sympathize with others. As children grow older, they learn to manage their emotions to block feelings of anxiety,
sadness, or frustration, and to delay gratification in order to achieve a goal.
Children need a combination of intellectual skills, motivational qualities, and social emotional skills to succeed in school.
They must be able to understand the feelings of others, control their own feelings and behaviors, and get along with
their peers and teachers. Children need to be able to cooperate, follow directions, demonstrate self-control, and “pay
attention.” One of the most important skills that children develop is self-control - the ability to manage one’s behavior
so as to resist impulses, maintain focus, and undertake tasks even if there are other more tempting options available.
Self-control motivates the ability to take on every task, so that the outcomes are not just how children get along with
one another but also how they can focus and learn in the classroom.
Social-emotional skills include the following:
• The child is able to understand and talk about his/her own feelings.
• The child understands the perspective of others and realizes that their feelings may be different from his/her own
feelings.
• The child is able to establish relationships with adults and maintains an ongoing friendship with at least one other
child.
• The child is able to enter a group successfully.
• The child is able to engage in and stay with an activity for a reasonable amount of time with minimal adult
support.
Social and emotional development involves the achievement of a set of skills. Among them is the ability to:
• Identify and understand one’s own feelings.
• Accurately read and comprehend emotional reactions from others.
• Manage strong emotions and their expression in a constructive manner.
• Control one’s own behavior.
• Develop compassion for others.
• Establish and maintain relationships.
Social and Emotional Behaviors in Preschool
Children with social and emotional problems enter kindergarten unable to learn because they cannot pay attention,
remember information on purpose, or act socially in a school environment. The result is growing numbers of children
who are hard to manage in the classroom. These children cannot get along with each other, follow directions, and are
impulsive. They show hostility and aggression in the classroom and on the playground. The problems begin before
kindergarten. In some studies as many as 32 percent of preschoolers in Head Start programs have behavioral problems.
Children lacking social and emotional skills suggest that teachers spend too much time trying to restrain unmanageable
children and less time teaching. Early childhood teachers report that they are extremely concerned about growing
classroom management problems, and that they are unprepared to handle them. Kindergarten teachers report that more
than half of their students come to school unprepared for learning academic subjects. If these problems are not dealt
with, the result can be growing aggression, behavioral problems and, for some, delinquency and crime through the
school years and into adolescence and adulthood.
Social and Emotional Aggression
Continual physical aggression, high-school dropout rates, adolescent delinquency, and antisocial behavior have all been
associated with early childhood conduct problems. The preschool years are a vulnerable period for learning to control
development of aggression. Children who display high levels of physical aggression in elementary school are at the
highest risk for taking part in violent behaviors as adolescents.
Researchers believe that children with difficult, disruptive behavior (poor social and emotional skills) are at risk for
these later problems for at least three reasons: (1) teachers find it harder to teach them, seeing them as less socially and
academically capable, and therefore provide them with less positive feedback; (2) peers reject them, which obstructs an
important opportunity for learning and emotional support; and (3) children faced with this rejection from peers and
teachers are likely to dislike school and learning, which leads to lower school attendance and poorer outcomes.
Difficult behavior exhibits itself early, even before children begin kindergarten; the pattern of rejection and negative
experiences begins early, too. The early experience of rejection can have lasting emotional and behavioral impacts
beyond elementary school, creating the problem even more difficult to reverse.
Developing Social and Emotional Skills
Promoting social and emotional development and preventing problems caused by inadequate development is clearly
important to individuals and to society. They begin with the relationships children form with the people around them,
including parents, caregivers, and peers. One characteristic of a successful person is his or her ability to live and work
peacefully and productively with others. Social capacity is the ability to interact positively within personal and family
relationships, as well as the ability to demonstrate positive concern and consideration. Emotionally healthy children
engage in positive behaviors, develop mutual friendships, and are more likely to find acceptance from their peers.
Through play, children learn how to work in teams and cooperate with others. Their behavior and interactions influence
the way in which teachers perceive them and the way they are treated by their peers. As early as preschool, the
relationships children develop with one another can have a lasting impact on academic achievement, because they can
contribute to more positive feelings about school and eagerness to engage in classroom activities, which can, in turn,
lead to higher levels of achievement.
Social Emotional Problems and Peer Relationships
Social interaction with peers builds upon and improves the rules and customs of social interaction that children first
encounter in their families. Although many adults assume that the influence of peers on adolescents is negative, the
repercussions of peer relationships are often more positive than negative. Peer relationships can provide cognitive,
social, and physical stimulation through mutual activities and conversations. Friendships in particular can provide
emotional security and compassion and can often serve as an additional source of support outside of the family,
especially in times of crisis.
Children must be provided an emotionally secure and safe environment that prevents any form of bullying or violence,
where they can be effective learners and integrate the development of social and emotional skills within all aspects of
school life. These skills include problem-solving, coping, conflict management/resolution and understanding and
managing feelings. Gaining social and emotional skills enables children to learn from teachers, make friends, express
thoughts and feelings, and cope with frustration. These kinds of skills, in turn, directly influence cognitive learning such
as early literacy, numeracy and language skills.
Early rejection by peers has been associated with persistent academic and social difficulties in elementary school. That
is why it is important to have skilled preschool teachers who can intervene when they see children having difficulties
with peers and help the children learn how to resolve conflicts, control emotions, and respond to the feelings of others.
Social Emotional Problems in the Family
Parents and families play a huge part in determining a child’s social and emotional development. Early relationships with
parents lay the foundation on which social ability and peer relationships are built. Parents who support positive
emotional development interact with their children affectionately; show consideration for their feelings, desires and
needs; express interest in their daily activities; respect their opinions; express pride in their achievements; and provide
support during times of anxiety. This encouragement significantly raises the probability that children will develop early
emotional capability, will be better prepared to enter school, and less likely to display behavior problems at home and at
school. This is why many preschool programs include a focus on parent involvement and parenting education.
Interactions with siblings are an important part of child development. These interactions influence the course of a child’
s social and moral development, including the development of good citizenship and good character. In general, having
an encouraging relationship with parents and siblings is important to positive adolescent development. Children who
disconnect from parental influence are at particular risk for delinquent activities and psychological problems.
Social and Emotional Support
The results of early childhood social-emotional problems may be a response from child distress and suffering, difficulty
with learning, trouble with play, poor peer interactions and sibling relationships, are all warnings of future mental health
problems. Nationally, fewer than 25% of children with clinical mental health problems receive treatment. Promoting
children’s social and emotional wellbeing can help improve their physical and mental health, performance at school and
assist with behavioral problems. A range of factors impact on how children feel, including their individual family
background and the community they live in, everyone needs to work together to agree effective strategies as part of a
team.
Children might need more focused instruction on skills such as: identifying and expressing emotions; self-control; social
problem solving; initiating and maintaining interactions; cooperative responding; strategies for handling disappointment
and anger; and friendship skills. Families of infants and young toddlers might need guidance and support for helping the
very young child regulate emotions or stress and understand the emotions of others.
Parents should consult with school staff regarding the social and emotional behavioral needs of their children. Once you
have contacted the school about concerns the following steps should be taken.
• A consultation with school staff regarding classroom and/or school approaches to behavior and to develop
positive behavior supports and interventions.
• Screening, evaluation, identification and referral for children displaying emotional disturbances.
• Planning and implementing appropriate academic and other educational supports.
• Measuring progress and improvement both for individuals and also for programs.
• Interventions for students with chronic behavior and emotional needs.
• Small group and/or individual counseling for such issues as social skills, anger control, etc.
• Development of expectations such as positive behavior and intervention, prevention of violence, crisis
planning and intervention, etc.
• Coordination and referral of children and families to community service agencies, related to mental health
needs.
When children have persistent challenging behavior that is not responsive to interventions, comprehensive interventions
are developed to resolve problem behavior and support the development of new skills. The process begins with
arranging the school staff that will develop and implement the child’s individualized education plan. At the center of the
team is the family and child’s teacher or other primary caregivers. The next step is to conduct a functional assessment
to gain a better understanding of the factors that are related to the child’s engagement in challenging behavior. The
individualized educational plan includes prevention strategies to address the triggers of challenging behavior;
replacement skills that alternatives to the challenging behavior; and strategies that ensure challenging behavior is not
reinforced or maintained. The individualized education plan is designed to address home, community, and classroom
routines where challenging behavior is occurring.
Social Convention
One of the really big problems that children encounter, that
everyone encounters in the process of growing up, is that
natural phenomenon involving a new force that presents itself
within a person at the onset of puberty. We are talking about
the powerful sexual force that manifests itself at the onset of
puberty around the age of 11 or 12 in the form of sexual
desire. Associated with this force, all mixed up with it, is
the phenomenon of "finding someone physically attractive" and
"falling in love", "being in love", etc. It is all part of the
same phenomenon. In fact, people fall into love and out of
love quite easily. "Falling in love" is really a kind of
temporary bewitchment, temporary enchantment, a temporary loss
of good sense. And involved also in this same phenomenon is
everyone's need for a companion of the opposite sex. A deep-
seated need. This whole phenomenon is nature's way of
perpetuating the species. It is a phenomenon that occurs in
all species. Behind it is the possibly partially obscured or
submerged wish to couple, procreate. Sexual desire can be like
an itch that torments. It is a new force within that dogs and
afflicts one, provoked and stimulated by imagination and
fantasy. It can be a desire that cries out for satisfaction,
an itch that demands appeasement. This entire phenomenon we
are talking about presents a lot of problems and difficulties
for a person. It is a brand new experience for a child and he
may not know quite how to handle it. Parents often don't want
to talk about it, don't quite know how to talk about it, and
the child learns about it from the effects it produces on
himself. The beginning of puberty is the end of innocence.
For along with this new force comes a realization that this
force within must be managed and controlled, since if is not
controlled, one would have a society of rampant promiscuity,
fornication and adultery; indeed a society of rampant rape,
child molestation and all kinds of ugly things. A usual way of
dealing with it is the appeasement of its incessant demands
through masturbation. The force brings frustration. For
thwarted desire produces frustration. And one knows the force
must be managed. The constantly recurring desire for sexual
intercourse coupled with the knowledge that sexual intercourse
produces babies and that you are not in any way ready in life
to have the responsibility of a baby produces inner conflict.
You are faced with the desire for something you want badly but
something that you know you must not allow, something your mind
tells you would be very bad for you, that would ruin your
future, your life. You are faced with a temptation to do
something that could be like a poison pill that could destroy
you. What a dilemma! That is life. An introduction to the
real world. In addition, you know God has stated that
fornication and adultery are sins, that fornicators and
adulterers will be punished by eternal hell. Thus this new
force brings a need for self-discipline. It creates a need for
restraint where restraint is difficult. Since it will be a
number of years yet before you will be in a position to marry
and have children you are faced with the problem of dealing
with this force by denying, thwarting and managing it for a
number of years. Thus much perseverance and patience is
required. It is a difficult task. All of this represents a
continuing, day to day problem of adolescent youth. It is
youth's first real encounter with temptation and the real need
to resist it. Many in our age do not resist it. They
foolishly follow their sexual inclinations, and end up having
babies or getting abortions. Or they take birth control pills.
They become promiscuous, having sex with multiple partners.
They follow the happy, easy way and others such as parents or
government take on the responsibilities that ought to be
theirs, the responsibilities of rearing and supporting the
illegitimate children that they beget and are not in a position
to rear. By taking the easy road, indulging their base
appetites and desires at a young age, they mess up their own
lives and place an unfair burden on others. They wrong others,
including their illegitimate children who are deserving of a
legitimate mother and father and a proper upbringing. And in
following the easy road of self-indulgence they build up habits
of sexual promiscuity that they will probably carry with them
the rest of their lives, even if they should eventually get
married.
Considering the problem that adolescent youth faces in dealing
with this problem reason and sense would call for societal
customs and practices that would assist teenagers in dealing
with the problem. If a person is overweight and is trying to
lose weight one does not place a chocolate cake under his nose.
If one is seriously attempting to avoid temptation one does not
put himself into situations producing temptation. A sensible
society could help a teenager in dealing with this problem.
Common sense would require social conventions and practices
that do not allow teenage youth of opposing sex to be alone
together. Common sense would require strict chaperoning of
youth. In a moral society parents and the adult world would
insist on chaperoning of youth. A moral society would not give
youth automobiles and the freedom that our society gives them.
Our laxness in dealing with our youth reveals our lack of
morals and unconcern about our youth. A sensible and moral
society would not allow on public mass media programs that
glamorize illegitimate sex. Teenagers do what they think
everyone else is doing. If everyone else is taking the easy,
fun, self-indulgent road they will take it too. If it is
glamorized on TV and in the movies and everyone appears to be
doing it they will do it too. It may be the foolish road but
fools follow fools. They live by the "feeling" philosophy.
Let your feelings be your guide (as opposed to your mind). Do
what you want to do, what you feel like doing. Live life.
Enjoy it. Don't let sense, reason or concern for others get in
your way.
There are many who condone illicit sex. They contend that
asking people to restrain and abstain is simply asking too much
of a person. The incidence of illicit sex and illegitimate
births among teenagers in this country is very high (over 50%
for illicit sex). However, I observe that the incidence of
illicit sex among teenagers in some cultures is extremely low
(perhaps 1 or 2 percent). I am thinking of the Japanese. I
think this fact is very interesting. It suggests that it is
all in the social attitudes and values of a particular society,
all in the "want to". People can do what they want to do. It
is all about morality or lack of it. It is true that the
Christian cultures seem just unable to restrain themselves in
regard to illicit sex. I don't fault the Christian religion
itself. The Bible is very clear on the topic, the New
Testament is very clear. The problem lies in the pervasive
perversion and corruption of Christianity. Man never seems
able to stay on a straight line. He always deviates off.
Intellectual
Adaptive behavior can also be defined as the effectiveness or degree with which the individual meets the standards of personal independence and social responsibility expected of his age and social group.[1] Adaptive behavior also refers to the typical performance of individuals without disabilities in meeting environmental expectations. Adaptive behavior changes according to a person’s age, cultural expectations, and environmental demands.
Behavior scales
To determine a student’s adaptive behavior capacities, professionals focus on the student’s conceptual skills, social skills, and practical skills. To measure adaptive skills, professionals use adaptive behavior scales that have been normed on individuals with and without disabilities. Most adaptive behavior scales are completed by interviewing a parent, a teacher, or another individual who is familiar with the student’s daily activities. Students may have a combination of strengths and needs in any or all of the areas regarding conceptual, social and practical skills.
Mental retardation/intellectual disability is significantly subaverage intellectual functioning present from birth or early infancy, causing limitations in the ability to conduct normal activities of daily living.
• Mental retardation/intellectual disability (MR/ID) can be genetic or the result of a disorder that interferes with brain development.
• Most children with MR/ID do not develop noticeable symptoms until they are in preschool.
• The diagnosis is based on the results of formal testing.
• A child's life expectancy is based on the extent of mental and physical problems.
• Proper prenatal care lowers the risk of having a child with MR/ID.
• Support from many specialists, therapy, and special education help children achieve the highest level of functioning possible.
The long-used term “mental retardation” has acquired an undesirable social stigma. Because of this stigma, doctors and health care practitioners have begun replacing it with the term "intellectual disability." Because this change is recent, the term "mental retardation/intellectual disability" (MR/ID) is used to mark the transition in terminology.
MR/ID is not a specific medical disorder like pneumonia or strep throat, and it is not a mental health disorder. People with MR/ID have significantly below average intellectual functioning that limits their ability to cope with two or more activities of normal daily living (adaptive skills). These activities include the ability to communicate; live at home; take care of oneself, including making decisions; participate in leisure, social, school, and work activities; and be aware of personal health and safety.
People with MR/ID have varying degrees of impairment. While recognizing each person's individuality, doctors find it helpful to classify a person's level of functioning. Intellectual functioning levels can be based on the results of developmental quotient (DQ) tests and intelligence quotient (IQ) tests or on the level of support needed. Support is categorized as intermittent, limited, extensive, or pervasive. Intermittent means occasional support; limited means support such as a day program in a sheltered workshop; extensive means daily, ongoing support; and pervasive means a high level of support for all activities of daily living, possibly including full-time nursing care.
Based only on IQ test scores, about 3% of the total population are considered to have MR/ID. However, if classification is based on the need for support, only about 1% of people are classified as having significant mental (cognitive) limitation.
Emotional problems in children
Emotional problems in children have become more widely recognized. A child's emotional problem can become a chronic problem if it's not attended to properly and in a timely manner. Many adult emotional problems can also affect children, but these problems may not be as easily recognized in children. Some emotional problems in children can be treated quite easily, but some require long-term care that can be complicated.
Childhood Bipolar Disorder
1. Childhood bipolar disorder is an emotional problem that can affect children. This childhood emotional problem can be hard to diagnose, because its symptoms are also symptoms of many other childhood emotional problems. Common symptoms include mood swings, irritability, episodes of extreme happiness and episodes of severe depression. Childhood bipolar disorder is a serious condition and should be treated as such. Treatment most often includes a combination of medication (sometimes more than one) and behavior therapy (teaching the child how to handle certain situations better).
Childhood Depression
2. Childhood depression is an emotional problem that can affect children. This childhood emotional problem is considered serious, but it can be difficult to diagnose because its symptoms are not unique. Common symptoms include irritability, fatigue, hopelessness, social withdrawal and poor performance in school. Childhood depression is most often treated with medication and behavior therapy.
Autism
3. Autism is an emotional problem that can affect children. This childhood emotional problem is often serious and consists of three distinctive behaviors. These autism behaviors include trouble interacting socially, obsessive and competitive behavior and difficulty with nonverbal and verbal communication. Medications (often more than one) and behavioral and educational therapies and interventions are used to treat autism. Family counseling is also used to help families learn about autistic children and to help them cope.
Childhood Schizophrenia
4. Childhood schizophrenia is an emotional problem that can affect children. This emotional disorder often affects a child's ability to develop normal social, educational and emotional skills and habits. Children with emotional disorder often have difficulty performing daily tasks, think and act irrationally and have delusions and hallucinations. Childhood schizophrenia is most often treated with a variety of treatments including medications (most often antipsychotics) and psychotherapy (teaches the child to cope with the illness and its challenges).
Tourette Syndrome
5. Tourette syndrome is an emotional problem that can affect children. This emotional problem is also considered a neurological disorder. Tourette syndrome is characterized by stereotyped and repetitive vocalizations and involuntary movements referred to as tics. Tourette syndrome is most often treated with a combination of medication and psychotherapy.
Physical
A recurrent theme of this year's AAFP Scientific Assembly was the evaluation and management of behavior problems in childhood. A series of talks focused on this issue and was led off by Dr. Barbara Howard's entertaining review of common behavioral problems encountered among children between ages 0 and 5 years.[1] Dr. Howard is Assistant Professor in Pediatrics at Johns Hopkins Medical Center and Co-Director of The Center for Promotion of Child Development through Primary Care. She noted that between 25% and 50% of physician visits for pediatric problems are behavioral, and 90% of parents with a child between the ages of 2 and 4 have some concern regarding their child's behavior.
Overall, Dr. Howard stressed the importance of "state regulation" for children, and the principal elements of this regulation are a standard routine of activities during the day and night as well as a consistent parental response to children's behaviors. Children with a history of insult to the central nervous system, lead poisoning, or exposure to substances in utero are particularly prone to behavioral problems without daily routines and consistent parental feedback.
Night awakening occurs in over 80% of children between the ages of 4 and 8 months, and 23.5% of children are not able to sleep for 6 consecutive hours at age 5 months.[2] New or problem night awakening frequently occurs after a change in the day's routine or some other stress. Dr. Howard recommends limiting naps to 2 hours per day and setting up bedtime routines. She then said, "Here comes the hard part: You have to let your baby cry a little bit." Dr. Howard recommends allowing the baby to cry for 5-10 minutes to help establish more mature sleep patterns.
Thumbsucking is a common practice among children and "may be a means of consoling themselves and also may improve gut motility and constipation," according to Dr. Howard. Nonetheless, thumbsucking may be less socially acceptable to some. "Who complains about thumbsucking?" asked Dr. Howard, "Grandma!"
Thumbsucking affects up to 31% of children and usually peaks between 1 and 2 years of age.[3] Parents should be relieved to learn that it generally does not affect dentition among children under the age of 6. For older children who continue to suck their thumbs, Dr. Howard recommends bribery or the use of thumb paint in a motivated child to dissuade thumbsucking.
Many toddlers may exhibit behavioral problems around mealtime, and Dr. Howard noted that this is probably "because autonomy is more important than hunger" during this stage of development. She discourages parents from chasing the toddler with food or bribing the child to encourage better eating habits. Instead, she recommends placement of nutritious finger foods on a low-lying table for the child to consume as desired. The child may be excused from the table at mealtime if he or she asks. Dr. Howard says that children will usually be drawn to the social experience of the mealtime table with the family after approximately 1 week of this therapy.
Dr. Howard closed with a discussion of toilet training, noting that "many children in other parts of the world begin toilet training by 1 year of age." However, children in the United States are generally encouraged to use the toilet only after they are able to control micturition and bowel movements to some extent and have full mobility. Dr. Howard stated that "there is no reason to start toilet training in a constipated kid" and recommends dietary fiber as a first-line agent to assure regularity. She also uses polyethylene glycol for children who refuse to eat fiber. She has had success using a strategy of room restriction for children having difficulty with toilet training. This strategy involves limitation of the child's movement to one room in the house (the room with the potty) until the child has a bowel movement. She noted that this strategy usually provides positive results within 2 days.
Colic is one of the most difficult behavioral problems to manage as a parent, and it warranted a separate lecture by Dr. Thomas Irons, Professor of Pediatrics at East Carolina University.[4] "I became interested in colic when I didn't know what to do about it with my own son," confessed Dr. Irons. He used the classic "rule of 3's" in defining colic as periods of intense crying for more than 3 hours per day on at least 3 days per week. He compared these statistics with an estimate that "the average baby cries an hour and three quarters per day." Colic generally resolves by 3 months of age. Dr. Irons noted that while no one treatment is effective for colic, research on therapy has demonstrated a placebo response rate of approximately 60%.[5] He encouraged parents to "take heart in the placebo effect" through treatments lacking a significant harmful potential for the baby, such as simethicone drops. Besides education and support from their family doctor, both Dr. Irons and Dr. Howard recommended "the 5 S's" as techniques which may help parents with crying infants:
• Swaddling, especially in combination with carrying the baby for a minimum of 3 hours per day;
• Side or prone positioning while the baby is being held;
• Shush -- use white noise to calm the baby;
• Sucking a pacifier; and
• Swing -- activating the vestibular system through a swing may reduce crying. Per Dr. Irons, "Run [the swing] as fast as it'll operate. Wind it up and let 'em go!"
Dr. Irons also noted some success associated with whey hydrosylate formula among children with colic who had received cow milk-based formula.[6] Parents may consider changing to this formula if their colicky infant is being bottle-fed. Dr. Howard suggested eliminating milk and cruciform vegetables from the mother's diet in colicky breastfed babies, as food allergy may play some role in colic.
Dr. Michelle May delivered an inspiring seminar regarding another problem behavior among children with which family physicians are all too familiar: overeating, lack of exercise, and obesity.[7] Dr. May is a family physician and the founder and medical director of Am I Hungry?, an adult weight-management program. She noted that 9 million children in the United States are overweight, and the prevalence has doubled in the last 2 decades.[8] She feels that identifying and treating pediatric obesity "is the hard stuff, and this is what we do as family physicians." Physicians should screen all children for overweight, using appropriate body mass index charts available at www.cdc.gov/growthcharts. Children above the 95th percentile for age-adjusted body mass index are considered overweight, although this should be interpreted with caution in adolescents because of varying rates of physical maturation.
"In this society, food is readily available, and there are many people with a financial interest in convincing us that we need to eat more than we do," stated Dr. May. She noted that portion sizes have increased by 25% to 50% over the last 2 decades. She also stated that "up to one third of food advertising contains misleading nutrition information," leading to a false sense of security for parents and children choosing foods poor in nutritional value. At the same time, less than half of schools offer physical education classes, and approximately 25% of children do not perform any physical activity outside of school.
While the negative societal influence on overweight in children runs deep, Dr. May relies on the fact that "children are born with the ability to regulate their own weight effortlessly." She offered the following advice for physicians counseling parents and children regarding diet:
• Don't reward eating. Do not praise or bribe toddlers for eating extra food, as this can establish a negative habit. Similarly, do not offer rewards for a clean plate at the end of the meal.
• Don't focus on ideal weight. Instead, set modest, achievable goals for overweight children.
• Monitor, but don't control. Dr. May finds that limiting dietary choices can be counterproductive, but focusing positively as a family on healthy foods produces healthier eating habits over the long term.[9]
• Don't give up on healthy foods. Dr. May has found that children may need to try a new food up to 10 times before accepting and enjoying it.
Regarding increasing activity, Dr. May suggested the following principles:
• Limit "screen time" (eg, television, computers, video games) to 2 hours per day.
• Address limitations in performing regular physical activity as a family, and strategize together how to overcome these barriers. The type of activity will vary from family to family but may be as simple as playing catch or taking a walk. Ideally, family physicians should be aware of community resources to help stimulate families to get active.
Overall, the series of lectures on children's behavior asserted the central role of family physicians in these health issues. Family doctors have the unique perspective of being able to assess the impact of family dynamics on children and counsel the family unit as a whole. These skills are highly valuable and will continue to be one of the strengths of the specialty.
Subscribe to:
Posts (Atom)